The main concern for most SARM users is the level of testosterone suppression they will experience after a cycle, and what they’ll have to do in order to reverse it.
For that purpose, we use what is known as a PCT, in the form of one or multiple SERMs, depending on the level of suppression experienced from the cycle.
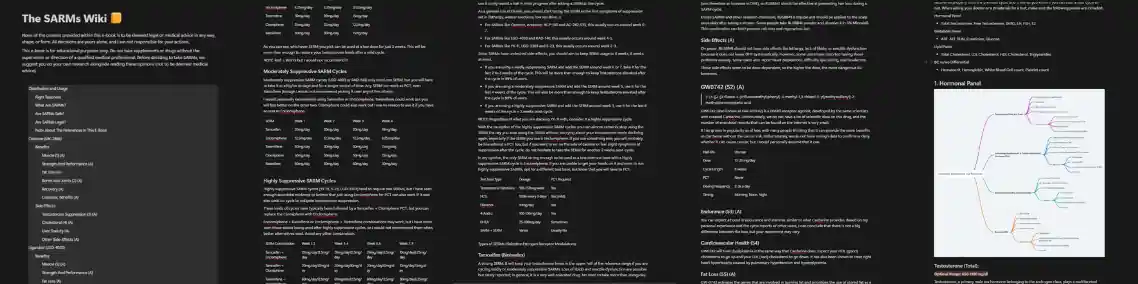
If we categorize the SARMs on the level of testosterone suppression they cause, we may divide them as:
IMPORTANT: Stacking multiple SARMs of any category should always be considered a highly suppressive cycle.
This article will delve into doing an effective PCT protocol after a moderately suppressive SARMs cycle with EITHER not BOTH RAD 140 or LGD 4033:
When looking into moderately suppressive SARMs, namely RAD 140 and LGD 4033, a PCT will almost always necessary. We know this based on countless clinical trials and heaps of empirical evidence.
Of course, there are outliners who can get away without doing a PCT but they are a minority and you should assume you’re not one of them.
So how do you go about assessing the level of suppression of a cycle?
Firstly this should never be left decided on speculation. Instead it should be done by carefully monitoring how you feel, and by doing a blood test of your hormonal panel, or at least your free test and LH.
So here’s how to determine whether PCT is necessary with and without bloodwork.
If you for whatever reason don’t do bloodwork you could probably get away without a PCT but only if you feel good, experience no sexual issues, and have no symptoms of low Testosterone – but I would still advise you to run a PCT for your own peace of mind anyways.
If you feel suppressed, or experience any symptoms of low testosterone, you should do a PCT.
Bloodwork is the only accurate way to determine whether a PCT is warranted or not. You will need to test for the following markers:
If your blood test shows that your Total Testosterone and LH levels are below the normal range, you’ll need a PCT, no matter how you feel. If they are within the normal range (even if they are close to the low end), you can probably skip a PCT. But if you still feel suppressed despite having normal levels, do a PCT anyway to feel better faster.
Once you determine that you need a PCT, the protocol itself is very straightforward:
Instructions:
I would personally recommend Enclomiphene or Tamoxifen as you will feel your best on either one of them. Toremifene would be my second option. I would avoid Clomiphene as Enclomiphene is a much better option. And finally Raloxifene would be my least favorable choice.
If you want to read more about why I’ve made these recommendations read this article on SERMs for bodybuilding.
On another note, you could also opt for an alternative approach and take the SERM on cycle as a non suppressive test base. This is a form of test base known as a SARM + SERM.
| WEEK 1 | WEEK 2 | WEEK 3 | WEEK 4 | |
| TAMOXIFEN | 20mg/day | 20mg/day | 20mg/day | 10mg/day |
| ENCLOMIPHENE | 12.5mg/day | 12.5mg/day | 12.5mg/day | 6.25mg/day |
| TOREMIFENE | 30mg/day | 30mg/day | 30mg/day | 15mg/day |
| CLOMIPHENE | 50mg/day | 50mg/day | 50mg/day | 25mg/day |
| RALOXIFENE | 60mg/day | 60mg/day | 60mg/day | 30mg/day |
Wrapping up, that’s all you need to know about running a PCT after a moderately suppressive SARM (either RAD 140 or LGD 4033). If you have more specific questions I urge you to send me a DM on Instagram @pathofpeds. Hope you found this useful.
premium resources
Everything you would ever want or need to know about SARMs to use and recover from them. Also includes other research chemicals.
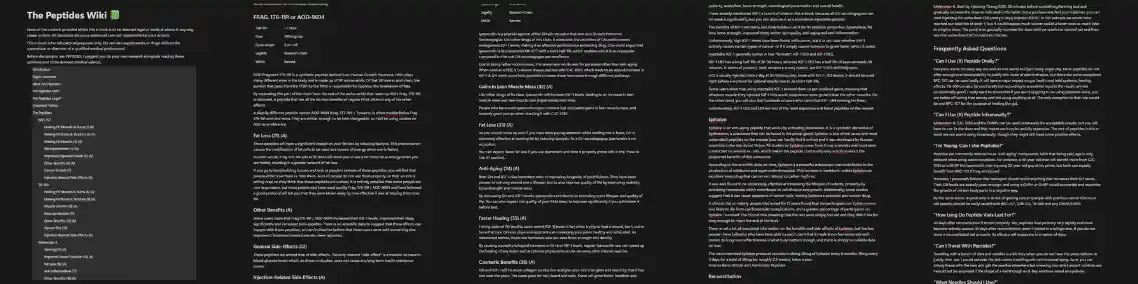
An all-in-one guide that will teach you how each of the peptides works, how you can use them and find the perfect one (or stack) to reach your goals.
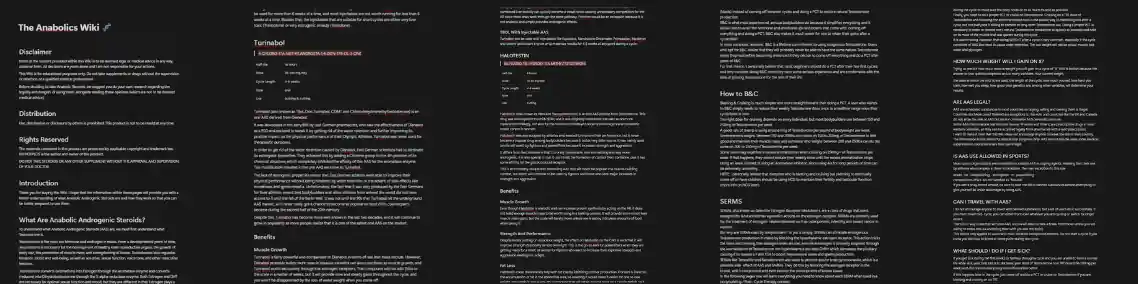
Wish there was ONE comprehensive, easy-to-read guide to get you fully informed on the safe and effective use of anabolic steroids?

Improve penile function, get harder fuller and longer-lasting erections, increase stamina in bed and last longer, go more rounds. All the good stuff.

A summary of everything you NEED to know about using PHs as safely as possible, supplements to stay as healthy as possible during cycles and how to recover (PCT).
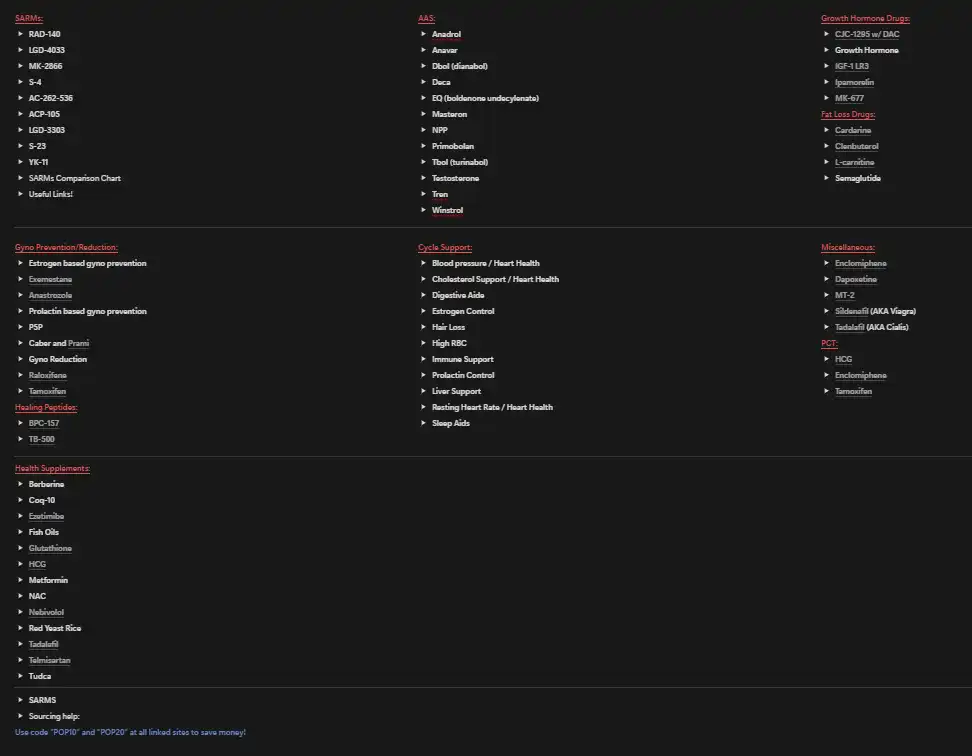
A document I originally made for my clients. A neat map to the sphere of PEDs and supplements.
You'll receive the link and a once-a-week PED-related article in your inbox upon subscribing.
A special gift to all my email subscribers. The PED Dictionary is a DOC designed to help you navigate the world of enhanced bodybuilding. A game changer for beginners that want to learn more but don't know where to start, and a must-have handbook for even the most advanced enhanced researchers.




