The best time to take SARMs depends on the SARMs’ half-life—the time necessary for a compound’s active substance to reduce by half in your body.
Dosages are to be timed precisely with the goal of achieving stable blood serum concentrations based on the compounds’ half-life.
If a SARM has a half-life of 24 hours, it would be ideal to take it at least once every 24 hours. Otherwise, you would experience peaks and valleys, failing to achieve stable blood concentrations of the SARM and somewhat compromising the effects.
Here is the best time to take each SARM based on the latest clinical data underlining the half-life. For chemicals that have an undefined half-life, I am referencing the administration times from their clinical trials. You will find the corresponding studies to each claim at the bottom of this article by looking at the number in parentheses.
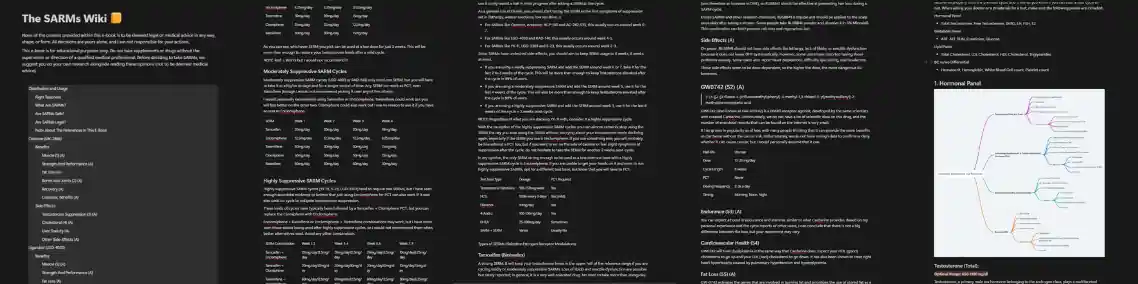
The best time to take Ostarine is in the morning, the same time every day. We know this based on its half-life, which is clinically proven to be 24 hours. [1]
The best time to take Ligandrol is in the morning, the same time every day. We know this based on its half-life, which is proven to be 24-36 hours. [2]
The best time to take Testolone is in the morning, the same time every day. We know this based on its half-life, which is proven to be 60 hours. [3]
Preclinical data (animal studies) on Andarine suggests that the half-life in humans is only 4 hours. [1]
But, that estimate is widely considered inaccurate and the real half-life of Andarine is thought to be in the range of 24-76 hours. This is based on thousands of anecdotal reports of experiencing the vision side effects days after their last dose of S4. This suggests the half-life is way longer than 4 hours.
Needless to say, in instances such as S4 where the half-life is not clinically proven, the safest way to ensure stable active substance levels is to split up the dosage across the day ideally on two to three separate occasions.
S-23, just like S4, has an undefined and clinically unknown half-life. It’s never been clinically tested on humans, and its half-life in rats is 11.9 hours. [5]
The half-life in humans can be deduced with a mathematical estimation, or preferably a clinical study.
For the time being, the ideal dosing regimen for S-23 would be to split the dose up and take it on two to three separate occasions throughout the day in order to achieve stable blood serum concentrations.
YK11’s half-life is clinically unknown, so splitting the dose throughout the day would be ideal to achieve stable blood serum concentrations.
LGD-3303’s half-life is clinically unknown. Knowing this, the ideal dosing regimen and best time to take LGD-3303 would be on two to three separate occasions throughout the day in order to achieve stable blood serum concentrations.
ACP-105’s half-life is clinically unknown. The ideal dosing regimen for it would be to split the dose into two to three occasions across the day to achieve stable blood serum concentrations.
AC-262-536’s half-life is also clinically unknown. The ideal dosing regimen for it would be to split up the dose into two to three occasions across the day to achieve stable blood serum concentrations.
Clinical data on Cardarine never revealed its half-life; however, all human trials had a once-daily dose schedule. [6]
So, we may conclude that Cardarine has a half-life of around 24 hours, and the best practice would be to follow what has been done in the trials.
Stenabolic’s half-life is clinically unknown. The best time to take it would be on multiple occasions throughout the day in order to ensure stable blood serum concentrations at all times.
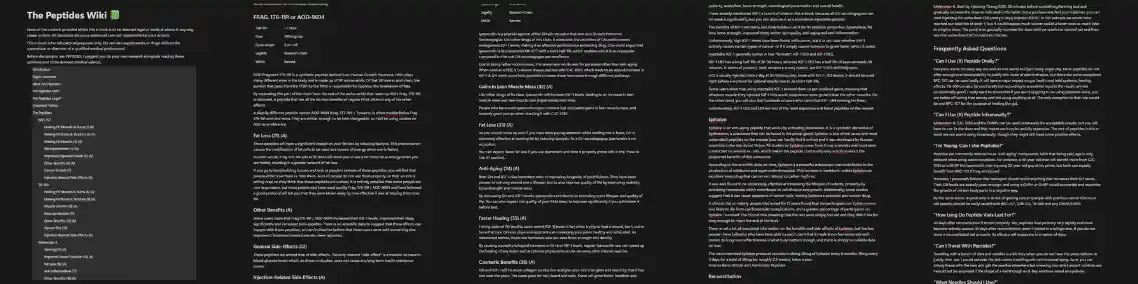
The terminal half-life of MK-677 is 4.7 hours, with IGF-1 levels remaining elevated for up to 24 hours. Once per day, dosing of MK-677 is a viable frequency of administration across the clinical studies to date. [6]
The timing may vary from morning to night depending on why you’re using MK677. If you’re using it to leverage its fat loss benefits, take it at night so you don’t have to deal with the increase in hunger. Otherwise, take it in the morning.
The half-life of RU-58841 was found to be 1 hour in an in vivo study. [4]
GW0742’s half-life is clinically unknown. The best time to take it would be on multiple occasions throughout the day in order to ensure stable blood serum concentrations at all times.
Many of the SARMs and other research chemicals on this list have clinical data and evidence on their half-lives in humans, which makes dosing them at the proper times much easier.
Others, like GW0742, S23, YK11, S4, MK677, ACP-105, AC-262-536, etc., are not as thoroughly researched, and the only data we have on their half-life is preclinical and anecdotal.
Fortunately, thousands upon thousands of users have recorded their personal experiences with them, so we have a good idea of how long their half-life might be, as well as when and how often we should take them.
premium resources
Everything you would ever want or need to know about SARMs to use and recover from them. Also includes other research chemicals.
An all-in-one guide that will teach you how each of the peptides works, how you can use them and find the perfect one (or stack) to reach your goals.
Wish there was ONE comprehensive, easy-to-read guide to get you fully informed on the safe and effective use of anabolic steroids?

Improve penile function, get harder fuller and longer-lasting erections, increase stamina in bed and last longer, go more rounds. All the good stuff.

A summary of everything you NEED to know about using PHs as safely as possible, supplements to stay as healthy as possible during cycles and how to recover (PCT).
A document I originally made for my clients. A neat map to the sphere of PEDs and supplements.
You'll receive the link and a once-a-week PED-related article in your inbox upon subscribing.
A special gift to all my email subscribers. The PED Dictionary is a DOC designed to help you navigate the world of enhanced bodybuilding. A game changer for beginners that want to learn more but don't know where to start, and a must-have handbook for even the most advanced enhanced researchers.




