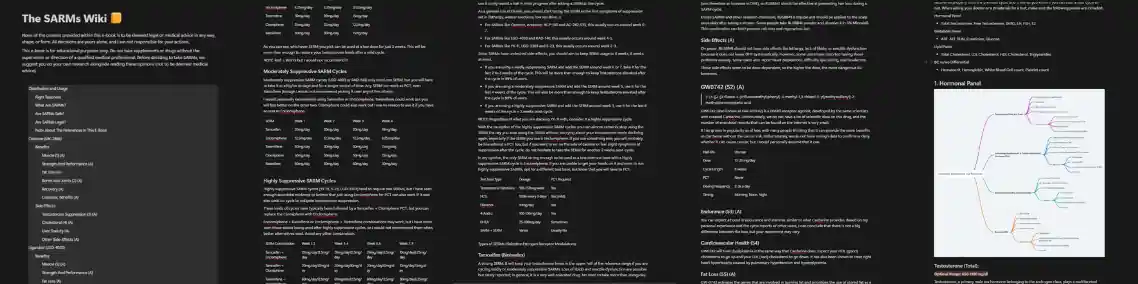
Most users going into SARMs over AAS (anabolic-androgenic-steroids) do so in order to preserve their natural testosterone production, and avoid going through a long and painful recovery phase. As such the first SARMs they look at are the ones that are known to be the most mild in terms of testosterone suppression:
This article is a comprehensive PCT guide for these SARMs. It is based on the latest academic data on said SARMs, the careful analysis of thousands of anecdotal reports online, and my own experiments with myself and over 500 lifetime clients in conditions deemed as controlled as possible. Take note.
Ostarine, S-4, ACP-105, and AC-262-536 rarely cause a level of testosterone suppression that warrants the need for a PCT (post-cycle-therapy) with a SERM (selective-estrogen-receptor-modulator). These are known as some of the least suppressive SARMs, and most users experience a level of suppression that is recoverable naturally
After a cycle of either one you can expect your endogenous Testosterone levels to be ~ 50% of what they were before your cycle.
This estimation is the average based on empirical data of post-cycle bloodwork results I’ve looked at. Most people recover their natural Testosterone levels back to or close to their baseline within a month.
But, this is not the case for everyone. As I’ve observed in many anecdotal cases, some users do in fact require a PCT. Typically these users already had low testosterone levels, and we’re not in the ideal spot for a cycle. I say typically, because it is not always the case. Individual response plays a key role. This is why you should always have a SERM at hand no matter how confident you are in your body’s natural ability to recover – just in case.
Mildly suppressive SARMs are a bit tricky when it comes to determining whether a PCT is neccessary. It always comes down to bloodwork.
Post cycle bloodwork is the most accurate way to determine whether you need to PCT after a cycle of:
If you for some reason cannot, or refuse to do bloodwork, then you could probably skip a PCT unless you feel the symptoms of suppression near the end and after your cycle. These include:
Looking at your bloodwork, you should run a PCT if:
Once you determine that you need a PCT, this is the protocol that you will follow:
Any of the SERMs can work as a PCT for mildly suppressive SARMs. Though, I recommend picking between Tamoxifen, Toremifene or Enclomiphene for optimal results.
As said any of the SERMs will be effective at restoring your testosterone levels to their baseline even at a low dose for 3 weeks after your cycle.
These SARMs are mild, and you most probably will not need to PCT. Though you can never know for sure, so it’s always smart to do bloodwork and have a SERM at hand just incase. And of course, the higher the dose, and the longer you run any of these SARMs, the probability that you will need to PCT after your cycle is higher.
Happy cycling.
premium resources
Everything you would ever want or need to know about SARMs to use and recover from them. Also includes other research chemicals.
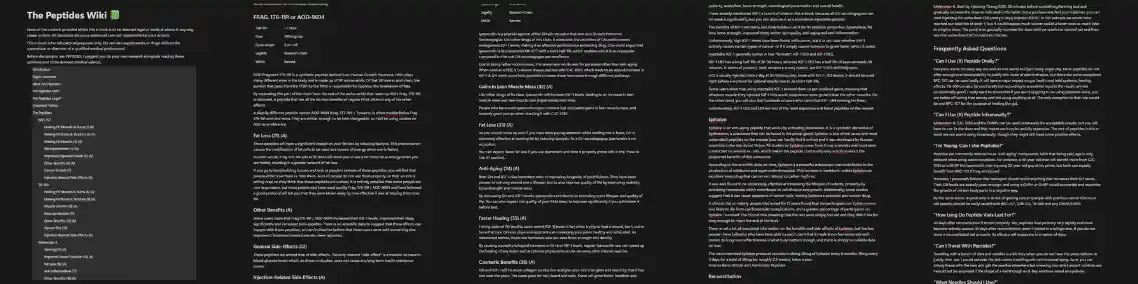
An all-in-one guide that will teach you how each of the peptides works, how you can use them and find the perfect one (or stack) to reach your goals.
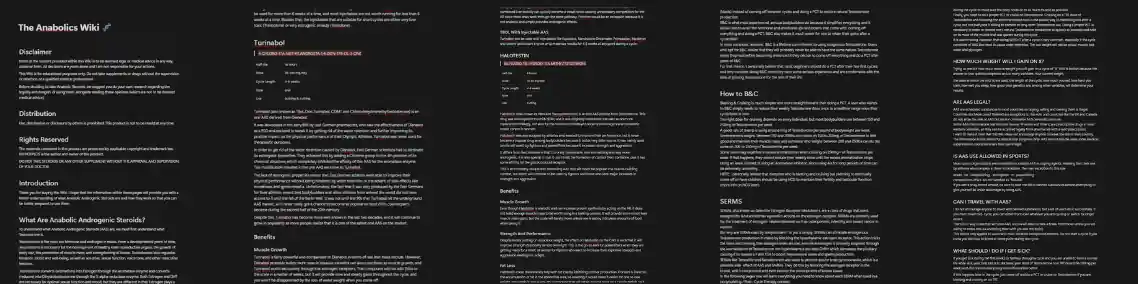
Wish there was ONE comprehensive, easy-to-read guide to get you fully informed on the safe and effective use of anabolic steroids?

Improve penile function, get harder fuller and longer-lasting erections, increase stamina in bed and last longer, go more rounds. All the good stuff.

A summary of everything you NEED to know about using PHs as safely as possible, supplements to stay as healthy as possible during cycles and how to recover (PCT).
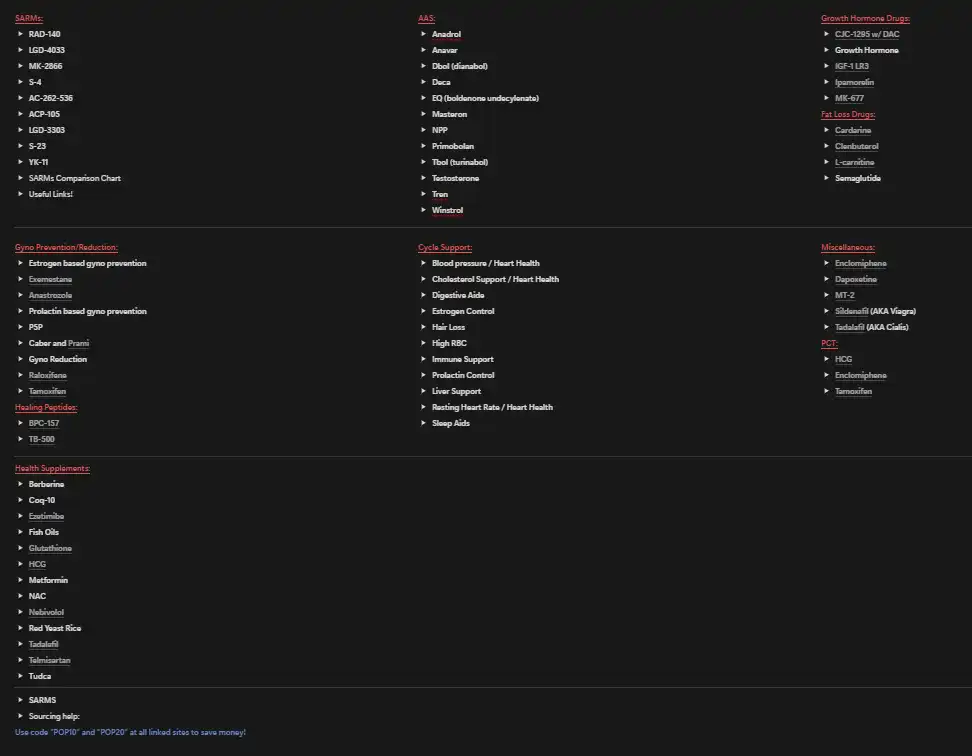
A document I originally made for my clients. A neat map to the sphere of PEDs and supplements.
You'll receive the link and a once-a-week PED-related article in your inbox upon subscribing.
A special gift to all my email subscribers. The PED Dictionary is a DOC designed to help you navigate the world of enhanced bodybuilding. A game changer for beginners that want to learn more but don't know where to start, and a must-have handbook for even the most advanced enhanced researchers.




